PENBRAYA™
(meningococcal groups A, B, C, W, and Y vaccine)
Find PENBRAYA™ medical information:
Find PENBRAYA™ medical information:
PENBRAYA™ Quick Finder
17 PATIENT COUNSELING INFORMATION
17 PATIENT COUNSELING INFORMATION
Prior to administration of PENBRAYA:
- •
- Inform vaccine recipient of the potential benefits and risks of vaccination with PENBRAYA.
- •
- Advise vaccine recipient to report any adverse events to their healthcare provider or to the Vaccine Adverse Event Reporting System at 1-800-822-7967 and https://vaers.hhs.gov/.
This product’s labeling may have been updated. For the most recent prescribing information, please visit https://dailymed.nlm.nih.gov/dailymed/.
Manufactured by:
Pfizer Ireland Pharmaceuticals
Ringaskiddy, Cork, Ireland
US License No. 2060

LAB-1512-4.0
Highlights
HIGHLIGHTS OF PRESCRIBING INFORMATIONThese highlights do not include all the information needed to use PENBRAYA safely and effectively. See full prescribing information for PENBRAYA. PENBRAYA (Meningococcal Groups A, B, C, W, and Y Vaccine), suspension for intramuscular injection Initial U.S. Approval: 2023 INDICATIONS AND USAGEPENBRAYA is indicated for active immunization to prevent invasive disease caused by Neisseria meningitidis serogroups A, B, C, W, and Y. PENBRAYA is approved for use in individuals 10 through 25 years of age. (1) DOSAGE AND ADMINISTRATIONDOSAGE FORMS AND STRENGTHSPENBRAYA is a suspension for injection. A single dose after reconstitution is approximately 0.5 mL. (3) CONTRAINDICATIONSSevere allergic reaction (e.g., anaphylaxis) to any component of PENBRAYA. (4) ADVERSE REACTIONSThe most commonly reported (≥15%) solicited adverse reactions after Dose 1 and Dose 2, respectively, were pain at the injection site (89% and 84%), fatigue (52% and 48%), headache (47% and 40%), muscle pain (26% and 23%), injection site redness (26% and 23%), injection site swelling (25% and 24%), joint pain (20% and 18%), and chills (20% and 16%). (6) To report SUSPECTED ADVERSE REACTIONS, contact Pfizer Inc. at 1-800-438-1985 or VAERS at 1-800-822-7967 or http://vaers.hhs.gov. See 17 for PATIENT COUNSELING INFORMATION. Revised: 11/2024 |
Indications and Usage
Dosage and Administration
2 DOSAGE AND ADMINISTRATION
For intramuscular use only.
2.2 Preparation
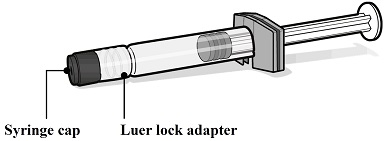
PENBRAYA is supplied in a kit that includes a vial of Lyophilized MenACWY Component (a sterile white powder), a prefilled syringe containing the MenB Component and a vial adapter.
To form PENBRAYA, reconstitute the Lyophilized MenACWY Component with the MenB Component as described in the instructions below.




2.3 Administration
For intramuscular use only.
After reconstitution, PENBRAYA is a homogeneous white suspension. If the vaccine is not a homogenous suspension, shake to resuspend prior to administration. Parenteral drug products should be inspected visually for particulate matter and discoloration prior to administration, whenever solution and container permit. Discard if either condition is present.
Administer PENBRAYA immediately or store between 2°C and 30°C (36°F and 86°F) and use within 4 hours. Discard reconstituted vaccine if not used within 4 hours.
Dosage Forms and Strengths
Contraindications
4 CONTRAINDICATIONS
Do not administer PENBRAYA to individuals with a history of severe allergic reaction (e.g., anaphylaxis) to any component of PENBRAYA [see Description (11)].
Warnings and Precautions
5 WARNINGS AND PRECAUTIONS
5.1 Management of Acute Allergic Reactions
Appropriate medical treatment used to manage immediate allergic reactions must be immediately available in the event an anaphylactic reaction occurs following administration of PENBRAYA.
5.2 Syncope
Syncope (fainting) may occur in association with administration of injectable vaccines, including PENBRAYA. Procedures should be in place to avoid injury from fainting.
5.3 Altered Immunocompetence
Reduced Immune Response
Some individuals with altered immunocompetence may have reduced immune responses to PENBRAYA.
Complement Deficiency
Individuals with certain complement deficiencies and individuals receiving treatment that inhibits terminal complement activation are at increased risk for invasive disease caused by N. meningitidis groups A, B, C, W, and Y, even if they develop antibodies following vaccination with PENBRAYA [see Clinical Pharmacology (12.1)].
5.4 Limitations of Vaccine Effectiveness
Vaccination with PENBRAYA may not protect all vaccine recipients.
5.5 Tetanus Immunization
Vaccination with PENBRAYA does not substitute for vaccination with a tetanus toxoid containing vaccine to prevent tetanus.
5.6 Guillain-Barré Syndrome
Guillain-Barré syndrome (GBS) has been reported in temporal relationship following administration of another U.S.-licensed meningococcal quadrivalent polysaccharide conjugate vaccine. The decision by the healthcare professional to administer PENBRAYA to persons with a history of GBS should take into account the expected benefits and potential risks.
Adverse Reactions
6 ADVERSE REACTIONS
The most commonly reported (≥15%) solicited adverse reactions after Dose 1 and Dose 2, respectively, were pain at the injection site (89% and 84%), fatigue (52% and 48%), headache (47% and 40%), muscle pain (26% and 23%), injection site redness (26% and 23%), injection site swelling (25% and 24%), joint pain (20% and 18%), and chills (20% and 16%).
6.1 Clinical Trials Experience
Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a vaccine cannot be directly compared to rates in the clinical trials of another vaccine and may not reflect the rates observed in practice.
The safety of PENBRAYA in individuals 10 through 25 years of age was evaluated in 3 clinical studies (2 active-controlled and 1 non-controlled study). In the controlled studies, 2306 participants received at least 1 dose of PENBRAYA. Of 946 participants who had previously received a meningococcal conjugate vaccine (categorized as MenACWY conjugate vaccine-exposed), 802 participants had received 1 dose of any U.S.-licensed Meningococcal Groups A, C, W, and Y conjugate vaccine, 51 participants had received a non-U.S.-licensed monovalent Meningococcal Group C conjugate vaccine (MenC conjugate vaccine), and 93 participants had received an unspecified U.S.-licensed or non-U.S.-licensed MenACWY conjugate or a MenC conjugate vaccine at least 4 years prior to enrollment. In the non-controlled study, 300 participants received a single dose of PENBRAYA.
Study 1 (NCT04440163) was an active-controlled, observer-blinded, multicenter study in which participants 10 through 25 years of age in the U.S. and Europe received at least 1 dose of PENBRAYA (N=1763) or Meningococcal Group B Vaccine (Trumenba) (N=650) at 0 and 6 months. Meningococcal Groups A, C, Y, and W-135 Oligosaccharide Diphtheria CRM197 Conjugate Vaccine (MenACWY-CRM, GSK Vaccines, SRL) was concomitantly administered with Trumenba at Month 0. All participants were MenB vaccine-naïve. Both MenACWY conjugate vaccine-naïve and MenACWY conjugate vaccine-exposed participants were part of the study.
Study 2 (NCT03135834) was an active-controlled, observer-blinded, multicenter study in which participants 10 through 25 years of age in the U.S. and Europe received at least 1 dose of PENBRAYA (N=543) or Trumenba (N=1057) at 0 and 6 months. MenACWY-CRM was co-administered with Trumenba at Month 0. All participants were MenB vaccine-naïve. Both MenACWY conjugate vaccine-naïve and MenACWY conjugate vaccine-exposed participants were part of this study.
Study 3 (NCT04440176) was a descriptive non-controlled study in which participants 11 through 14 years of age in the U.S. received PENBRAYA 12 months apart. All participants were naïve to any meningococcal vaccine.
In Study 1 and Study 2, solicited local and systemic adverse reactions were monitored for 7 days after study vaccination using an electronic diary. In all studies, spontaneous reports of adverse events (AEs) were collected through at least 1 month after the last vaccination, and through 6 months after the last vaccination for serious adverse events (SAEs).
In controlled studies, demographic characteristics were generally similar with regard to gender, race, and ethnicity among participants who received PENBRAYA and those who received control (Trumenba and MenACWY-CRM). Among participants who received PENBRAYA in controlled studies, 47.4% were male, 79.4% were White, 10.2% were Black or African-American, 2.1% were Asian, and 2.6% were of other racial groups, and 21.6% were of Hispanic/Latino ethnicity.
Solicited Local and Systemic Adverse Reactions
Table 1 presents the solicited local adverse reactions and Table 2 presents the solicited systemic adverse reactions and use of antipyretic medication reported within 7 days following each dose of PENBRAYA in Study 1.
| Abbreviations: N = number of participants; MenACWY-CRM = meningococcal (serogroups A, C, W and Y) oligosaccharide diphtheria CRM197 conjugate vaccine; Trumenba = meningococcal serogroup B factor H binding protein. | ||||
| ||||
Injection Site Reactions | PENBRAYA | Trumenba + MenACWY-CRM† | ||
Dose 1 | Dose 2 | Dose 1 | Dose 2 | |
N=1724-1725 % | N=1456 % | N=630-631 % | N=529 % | |
Pain‡ | ||||
Any§ | 89.3 | 84.4 | 85.1 | 78.6 |
Mild | 32.3 | 29.1 | 31.1 | 33.1 |
Moderate | 49.4 | 48.8 | 47.7 | 40.3 |
Severe | 7.5 | 6.5 | 6.3 | 5.3 |
Redness¶ | ||||
Any§ | 25.9 | 23.2 | 19.5 | 14.7 |
Mild | 8.9 | 7.7 | 7.3 | 6.6 |
Moderate | 14.4 | 12.6 | 10.0 | 7.2 |
Severe | 2.6 | 3.0 | 2.2 | 0.9 |
Swelling¶ | ||||
Any§ | 25.0 | 24.2 | 21.4 | 14.7 |
Mild | 10.6 | 10.4 | 8.3 | 6.4 |
Moderate | 13.3 | 12.8 | 12.4 | 8.1 |
Severe | 1.2 | 1.0 | 0.8 | 0.2 |
| Abbreviations: N = number of participants; MenACWY-CRM = meningococcal (serogroups A, C, W and Y) oligosaccharide diphtheria CRM197 conjugate vaccine; Trumenba= meningococcal serogroup B factor H binding protein. | ||||
| ||||
Systemic Reactions | PENBRAYA | Trumenba + MenACWY-CRM* | ||
Dose 1 | Dose 2 | Dose 1 | Dose 2 | |
N=1739-1740 % | N=1459 % | N=638 % | N=532 % | |
Fever (≥38°C) | ||||
≥38.0°C | 5.9 | 2.4 | 5.8 | 1.5 |
38.0° to 38.4°C | 3.7 | 1.9 | 2.0 | 0.4 |
>38.4° to 38.9°C | 1.6 | 0.3 | 2.8 | 0.9 |
>38.9° to 40.0°C | 0.6 | 0.2 | 0.9 | 0.2 |
>40.0°C | 0.0 | 0.0 | 0.0 | 0.0 |
Vomiting† | ||||
Any‡ | 3.2 | 1.5 | 3.0 | 0.9 |
Mild | 2.5 | 1.4 | 2.0 | 0.8 |
Moderate | 0.6 | 0.1 | 0.9 | 0.2 |
Severe | 0.0 | 0.0 | 0.0 | 0.0 |
Diarrhea§ | ||||
Any‡ | 11.0 | 8.2 | 13.5 | 8.5 |
Mild | 8.7 | 6.9 | 11.9 | 6.0 |
Moderate | 2.0 | 1.4 | 1.6 | 2.4 |
Severe | 0.3 | 0.0 | 0.0 | 0.0 |
Headache¶ | ||||
Any‡ | 46.8 | 39.8 | 46.9 | 37.8 |
Mild | 25.7 | 21.3 | 24.5 | 21.1 |
Moderate | 19.2 | 16.8 | 20.4 | 16.2 |
Severe | 1.9 | 1.7 | 2.0 | 0.6 |
Fatigue¶ | ||||
Any‡ | 52.1 | 47.6 | 54.7 | 43.6 |
Mild | 23.5 | 22.8 | 25.7 | 22.0 |
Moderate | 25.5 | 21.8 | 25.7 | 19.9 |
Severe | 3.2 | 2.9 | 3.3 | 1.7 |
Chills¶ | ||||
Any‡ | 20.1 | 16.4 | 19.6 | 16.2 |
Mild | 12.6 | 9.9 | 10.2 | 8.8 |
Moderate | 6.7 | 6.0 | 7.8 | 5.8 |
Severe | 0.8 | 0.4 | 1.6 | 1.5 |
Muscle pain (other than muscle pain at the injection site)¶ | ||||
Any‡ | 25.7 | 22.8 | 27.4 | 22.2 |
Mild | 13.6 | 10.0 | 13.5 | 10.0 |
Moderate | 10.5 | 11.9 | 11.9 | 11.5 |
Severe | 1.6 | 0.8 | 2.0 | 0.8 |
Joint pain¶ | ||||
Any‡ | 20.2 | 18.3 | 22.6 | 15.6 |
Mild | 10.7 | 9.6 | 12.9 | 7.9 |
Moderate | 8.6 | 8.3 | 8.6 | 6.8 |
Severe | 1.0 | 0.4 | 1.1 | 0.9 |
Use of antipyretic medication | 29.5 | 25.1 | 28.1 | 20.5 |
Serious Adverse Events
In Study 1, during the 30 days after vaccination visit 1 (at 0 months), <0.1% (1/1763) of PENBRAYA and 0% (0/649) of Trumenba + MenACWY-CRM participants reported at least 1 SAE. During the 30 days after vaccination visit 2 (at 6 months), 0.1% (2/1558) of PENBRAYA and 0% (0/562) of Trumenba participants reported at least 1 SAE. None of the SAEs were determined to be related to PENBRAYA vaccination.
In Study 2, during the 30 days after vaccination visit 1 (at 0 months), 0.4% (2/543) of PENBRAYA and 0% (0/1057) of Trumenba + MenACWY-CRM participants reported at least 1 SAE. During the 30 days after vaccination visit 2 (at 6 months), 0.2% (1/486) of PENBRAYA and 0% (0/946) of Trumenba participants reported at least 1 SAE. None of the SAEs were determined to be related to PENBRAYA vaccination.
In non-controlled Study 3, no SAEs (0/294) were reported within 30 days after either vaccination (0, 12 months).
6.2 Postmarketing Experience
The postmarketing safety experience with Trumenba and a non-U.S.-licensed Meningococcal Groups A, C, W, and Y polysaccharide tetanus toxoid (TT) conjugate vaccine (MenACWY-TT vaccine; Pfizer Inc.) is relevant to PENBRAYA since PENBRAYA includes the same group A, C, W, and Y TT-conjugated polysaccharide components and MenB recombinant protein components. Because these events are reported voluntarily from a population of uncertain size, it is not possible to reliably estimate their frequency or establish a causal relationship to vaccination. The following adverse reactions have been spontaneously reported during postmarketing use of Trumenba and MenACWY-TT and may also be seen in postmarketing experience with PENBRAYA.
Immune System Disorders: allergic reactions, including anaphylaxis
Nervous System: syncope (fainting)
Use in Specific Populations
8 USE IN SPECIFIC POPULATIONS
8.1 Pregnancy
Pregnancy Exposure Registry
There is a pregnancy exposure registry that monitors pregnancy outcomes in individuals exposed to PENBRAYA during pregnancy. Individuals who received PENBRAYA during pregnancy are encouraged to contact, or have their healthcare provider contact, 1-877-390-2953 to enroll in or obtain information about the registry.
Risk Summary
All pregnancies have a risk of birth defect, loss, or other adverse outcomes. In the U.S. general population, the estimated background risk of major birth defects and miscarriage in clinically recognized pregnancies is 2% to 4% and 15% to 20%, respectively.
There are no clinical studies of PENBRAYA in pregnant individuals. Available human data on PENBRAYA administered to pregnant individuals are insufficient to inform vaccine-associated risks in pregnancy.
There were no developmental toxicity studies performed with PENBRAYA.
8.2 Lactation
Risk Summary
There are no data available to assess the effects of PENBRAYA on the breastfed infant or on milk production/excretion. The developmental and health benefits of breastfeeding should be considered along with the mother's clinical need for PENBRAYA and any potential adverse effects on the breastfed child from PENBRAYA or from the underlying maternal condition. For preventive vaccines, the underlying maternal condition is susceptibility to disease prevented by the vaccine.
8.4 Pediatric Use
The safety and effectiveness of PENBRAYA have not been established in individuals <10 years of age. In a clinical study, 90% of infants younger than 12 months of age who were vaccinated with a reduced dosage formulation of Trumenba had fever. PENBRAYA contains the same MenB component, in the same quantity, as Trumenba.
Description
11 DESCRIPTION
PENBRAYA (Meningococcal Groups A, B, C, W, and Y Vaccine) is a suspension for intramuscular injection. PENBRAYA is supplied as a sterile Lyophilized MenACWY Component to be reconstituted with the sterile MenB Component.
The Lyophilized MenACWY Component consists of N. meningitidis serogroups A, C, W, and Y polysaccharides individually conjugated to TT. The polysaccharide for each group is grown in media containing dextrose, salt, and yeast extract, then purified by precipitation and filtration. The TT is produced by fermentation of Clostridium tetani in dextrose, salts, and tryptone N1 peptone followed by formalin detoxification, then purified by a series of physicochemical steps. The serogroups A and C polysaccharides are individually microfluidized, activated with 1-cyano-4(dimethylamino)-pyridinium tetrafluoroborate (CDAP), derivatized with adipic acid dihydrazide (ADH), and then conjugated with TT in the presence of 1-ethyl-3-(3-dimethylaminopropyl)carbodiimide) (EDAC). The serogroups W and Y polysaccharides are individually microfluidized, activated with CDAP, and then conjugated with TT. The conjugates are purified by a series of physicochemical steps then sterile filtered. Trometamol/sucrose buffer is added, and the MenACWY-TT solution is lyophilized.
The MenB Component is a sterile suspension composed of 2 recombinant lipidated factor H binding protein (fHbp) variants from N. meningitidis serogroup B, 1 from fHbp subfamily A and 1 from fHbp subfamily B (A05 and B01, respectively). The proteins are individually produced in Escherichia coli. Production strains are grown to a specific density in chemically defined fermentation growth media without antibiotics or animal-derived components. The recombinant proteins are extracted from the production strains and purified through a series of column chromatography steps. Polysorbate 80 (PS80) is added and is present in the MenB Component.
Each approximately 0.5 mL dose of PENBRAYA contains N. meningitidis serogroup A, C, W, and Y polysaccharide (5 mcg each; 20 mcg total) conjugated to tetanus toxoid (44 mcg tetanus toxoid), 2 recombinant lipidated factor H binding protein variants from N. meningitidis serogroup B (60 mcg each; total of 120 mcg protein), L-histidine (0.78 mg) , trometamol (0.097 mg), sucrose (28 mg), aluminum phosphate (0.25 mg aluminum), sodium chloride (4.65 mg), and PS80 80 (0.018 mg) at pH 6.0.
PENBRAYA does not contain any preservatives.
Clinical Pharmacology
12 CLINICAL PHARMACOLOGY
12.1 Mechanism of Action
Protection against invasive meningococcal disease is conferred mainly by complement-mediated antibody-dependent killing of N. meningitidis.1 Vaccination with PENBRAYA induces the production of bactericidal antibodies specific to the capsular polysaccharides of N. meningitidis serogroups A, C, W, and Y and to fHbp subfamily A and B variants of N. meningitidis group B. The susceptibility of group B meningococci to bactericidal antibody is dependent upon both the antigenic similarity of the fHbp subfamily A or subfamily B vaccine antigen to the fHbp protein expressed by the bacterial strain and the amount of fHbp expressed at the bacterial surface.2
Nonclinical Toxicology
Clinical Studies
14 CLINICAL STUDIES
The effectiveness of PENBRAYA was assessed in Study 1 by measuring antibodies with assays that used human complement to assess serum bactericidal activity (hSBA). For serogroups A, C, W, and Y, one strain was utilized per group. For serogroup B, four meningococcal serogroup B strains expressing different fHbp variants that represent the A and B subfamilies of meningococcal serogroup B strains causing invasive disease in the U.S. and Europe were utilized. The proportions of subjects with a 4-fold or greater increase in hSBA titer for each strain, and the proportion of subjects with a titer greater than or equal to the lower limit of quantitation (LLOQ) of the assay for all four serogroup B strains (composite response) were assessed.
14.1 Immunogenicity
Study 1 was a Phase 3, randomized, active-controlled, observer-blinded, multicenter study in which participants 10 through 25 years of age in the U.S. and Europe received PENBRAYA at 0 and 6 months or Trumenba at 0 and 6 months and MenACWY-CRM at 0 months. All participants were MenB vaccine-naïve. Both MenACWY conjugate vaccine -naïve and MenACWY conjugate vaccine-exposed participants were part of the study.
Seroresponse for serogroups A, B, C, W, and Y and composite response for serogroup B following 2 doses of PENBRAYA in Study 1 are presented in Tables 3 and 4.
Among both ACWY-naïve and ACWY-exposed participants, seroresponse rates to serogroups A, C, W, and Y following 2 doses of PENBRAYA were demonstrated to be non-inferior to seroresponse rates following a single dose of MenACWY-CRM. Seroresponse and composite response rates to serogroup B primary strains among participants who received 2 doses of PENBRAYA were demonstrated to be non-inferior to seroresponse and composite response rates following 2 doses of Trumenba.
| Abbreviations: CI = confidence interval; hSBA = serum bactericidal assay using human complement; LLOQ = lower limit of quantitation; LOD = limit of detection; MenACWY-CRM = meningococcal (serogroups A, C, W and Y) oligosaccharide diphtheria CRM197 conjugate vaccine; Trumenba= meningococcal serogroup B factor H binding protein. | |||
| Note: The LLOQ is an hSBA titer = 1:16 for A22 and 1:8 for A56, B24, and B44 and serogroups A, C, W, and Y. | |||
| Note: Seroresponse is defined as the 4-fold increase as follows: (1) For participants with a baseline hSBA titer <1:4 (LOD), a 4-fold response was defined as an hSBA titer ≥1:16. (2) For participants with a baseline hSBA titer ≥ LOD and < LLOQ, a response is defined as an hSBA titer ≥4 times the LLOQ. (3) For participants with a baseline hSBA titer ≥ LLOQ, a response is defined as an hSBA titer ≥4 times the baseline titer. | |||
Serogroup | PENBRAYA % | Trumenba + MenACWY-CRM % | PENBRAYA – MenACWY-CRM Difference‡ |
N=439-451 (Naïve) N=376-387 (Exposed) | N=244-254 (Naïve) N=222-227 (Exposed) | Difference % (95% CI) | |
A | |||
ACWY-naïve | 97.8 | 95.3 | 2.5 (-0.2, 6.0) |
ACWY-exposed | 93.8 | 96.9 | -3.2 (-6.5, 0.5) |
C | |||
ACWY-naïve | 93.3 | 52.4 | 41.0 (34.4, 47.5) |
ACWY-exposed | 93.8 | 94.7 | -0.9 (-4.6, 3.3) |
W | |||
ACWY- naïve | 97.3 | 73.0 | 24.3 (18.8, 30.4) |
ACWY-exposed | 97.1 | 96.4 | 0.7 (-2.2, 4.3) |
Y | |||
ACWY- naïve | 94.4 | 70.6 | 23.8 (18.0, 30.1) |
ACWY-exposed | 93.0 | 93.7 | -0.7 (-4.6, 3.8) |
| Abbreviations: CI = confidence interval; hSBA = serum bactericidal assay using human complement; LLOQ = lower limit of quantitation; LOD = limit of detection; MenACWY-CRM = meningococcal (serogroups A, C, W and Y) oligosaccharide diphtheria CRM197 conjugate vaccine; Trumenba= meningococcal serogroup B factor H binding protein. | |||
| Note: The LLOQ is an hSBA titer = 1:16 for A22 and 1:8 for A56, B24, and B44 and serogroups A, C, W, and Y. | |||
| Note: Seroresponse is defined as the 4-fold increase as follows: (1) For participants with a baseline hSBA titer <1:4 (LOD), a 4-fold response was defined as an hSBA titer ≥1:16. (2) For participants with a baseline hSBA titer ≥ LOD and < LLOQ, a response is defined as an hSBA titer ≥4 times the LLOQ. (3) For participants with a baseline hSBA titer ≥ LLOQ, a response is defined as an hSBA titer ≥4 times the baseline titer. | |||
PENBRAYA % | Trumenba + MenACWY-CRM % | PENBRAYA – Trumenba Difference | |
Serogroup B Variant | N=755-845 | N=383-419 | Difference % (95% CI) |
Seroresponse‡ | |||
A22 | 83.0 | 79.0 | 4.0 (-0.7, 8.9) |
A56 | 95.9 | 94.5 | 1.4 (-1.0, 4.3) |
B24 | 68.1 | 57.2 | 10.9 (5.2, 16.6) |
B44 | 86.5 | 79.2 | 7.3 (2.9, 11.9) |
Composite§ | |||
Pre-Dose 1 | 1.2 | 2.0 | - |
Post-Dose 2 | 78.3 | 68.7 | 9.6 (4.2, 15.2) |
References
15 REFERENCES
- 1.
- Goldschneider I, Gotschlich EC, Artenstein MS. Human immunity to the meningococcus. I. The role of humoral antibodies. J Exp Med. (1969);129:1307–1326.
- 2.
- Wang X, et al. Prevalence and genetic diversity of candidate vaccine antigens among invasive Neisseria meningitidis isolates in the U.S. Vaccine 2011; 29:4739-4744.
How Supplied/Storage and Handling
16 HOW SUPPLIED/STORAGE AND HANDLING
16.1 How Supplied
PENBRAYA is supplied in a kit that includes a vial of Lyophilized MenACWY Component (NDC 0069-0271-01), a prefilled syringe containing MenB Component (NDC 0069-0332-01) and a vial adapter. The Lyophilized MenACWY Component is reconstituted with the MenB Component to form a single dose of PENBRAYA.
PENBRAYA is supplied in cartons of 1, 5, and 10 kits.
Carton: 1 kit | 0069-0600-01 |
Carton: 5 kits | 0069-0600-05 |
Carton: 10 kits | 0069-0600-10 |
The vial stopper and the syringe tip cap and plunger stopper are not made with natural rubber latex.
16.2 Storage Before Reconstitution
Store refrigerated at 2°C to 8°C (36°F to 46°F) in the original carton. During storage, a white deposit and clear supernatant may be observed in the prefilled syringe containing the MenB Component. Store the carton horizontally to minimize the time necessary to resuspend the MenB Component.
Do not freeze. Discard if the carton has been frozen.
Patient Counseling Information
17 PATIENT COUNSELING INFORMATION
Prior to administration of PENBRAYA:
- •
- Inform vaccine recipient of the potential benefits and risks of vaccination with PENBRAYA.
- •
- Advise vaccine recipient to report any adverse events to their healthcare provider or to the Vaccine Adverse Event Reporting System at 1-800-822-7967 and https://vaers.hhs.gov/.
This product’s labeling may have been updated. For the most recent prescribing information, please visit https://dailymed.nlm.nih.gov/dailymed/.
Manufactured by:
Pfizer Ireland Pharmaceuticals
Ringaskiddy, Cork, Ireland
US License No. 2060
LAB-1512-4.0
Resources
Didn’t find what you were looking for? Contact us.
Chat online with Pfizer Medical Information regarding your inquiry on a Pfizer medicine.
*Contact Medical Information. 9AM-5PM ET Monday to Friday; excluding holidays.
Report Adverse Event
Pfizer Safety
To report an adverse event related to the Pfizer-BioNTech COVID-19 Vaccine, and you are not part of a clinical trial* for this product, click the link below to submit your information:
Pfizer Safety Reporting Site*If you are involved in a clinical trial for this product, adverse events should be reported to your coordinating study site.
If you cannot use the above website, or would like to report an adverse event related to a different Pfizer product, please call Pfizer Safety at (800) 438-1985.
FDA Medwatch
You may also contact the U.S. Food and Drug Administration (FDA) directly to report adverse events or product quality concerns either online at www.fda.gov/medwatch or call (800) 822-7967.